Hypothéses sur les origines des troubles
Hypothèses Physiopathologiques
HISTORIQUE
De lAntiquité au XIXe siècle
Lhistoire des idées concernant lhystérie est très ancienne et est lune des
plus passionnantes de lhistoire de la médecine. Durant lantiquité grecque
(Hippocrate), lorigine du trouble se situait au niveau dun utérus « errant »
qui pouvait bloquer linflux nerveux et qui, par exemple, pouvait entraîner une
gêne respiratoire lorsquil migrait au niveau des poumons. Au Moyen Âge, ces
patientes étaient souvent considérées comme des sorcières, envoûtés par le
démon, et qui pouvaient être condamnées au bûcher. Thomas SYNDENHAM au XVIIe
siècle, à Londres, avait montré le caractère protéiforme et changeant de
lhystérie, avec des passages dun symptôme à un autre.
Le XIXe siècle
Il a fallu attendre le milieu du XIXe siècle pour que son origine cérébrale soit
reconnue (Pierre Briquet). Ce neurologue parisien a mis, en outre, en évidence
le rôle favorisant dexpériences traumatisantes anciennes. Un peu plus tard,
John Russel Reynolds à Londres, montre limportance des émotions et des « idées
» ou représentations dans lapparition des symptômes (avant de faire un
mouvement, il faut le programmer à partir dune idée). Toujours dans cette fin
du XIXe siècle, Jean Martin Charcot, neurologue à la Salpêtrière à Paris, essaie
dappliquer la méthode anatomo-clinique de la neurologie à lhystérie quil va
dabord considérer comme un problème purement neurologique. Il va émettre
lhypothèse très moderne d « une lésion fonctionnelle ». Cette lésion, il ne
pourra pas la voir en analysant les pièces anatomiques de cerveaux de patients
hystériques décédés. Cependant cette hypothèse se verra confirmée par les
données récentes de limagerie fonctionnelle cérébrale (voir ci-dessous).
Nayant pas trouvé de lésion fonctionnelle, il abandonnera progressivement
lapproche neurologique pour accorder une importance aux émotions et aux idées
(ou représentations le plus souvent inconscientes) : « une idée peut provoquer
une paralysie et lautre peut la guérir ». Il explique ainsi certaines
améliorations ou guérisons spontanées inattendues. Il va créer un laboratoire de
psychologie physiologique pour le psychiatre Pierre Janet qui va introduire en
concept qui deviendra majeur et dont nous reparlerons ci-dessous : le phénomène
de dissociation, cest-à-dire la capacité que le cerveau a de se « dissocier »,
de se fragmenter ou de se compartimentaliser, lors dune émotion forte, pouvant
entraîner les différents symptômes que lon rencontre dans les TNF. À titre
dexemple, lamnésie parfois observée lors dun traumatisme psychologique
important ou dun abus sexuel correspond à lexclusion de certains réseaux de la
mémoire du champ de la conscience.
Le XXe siècle
Le modèle conceptuel qui a eu le plus de notoriété au début du XXe siècle a été
celui de la « conversion hystérique », processus qui convertit une détresse
psychologique insupportable en symptômes physiques de façon à apaiser
langoisse. Sigmund Freud a modifié ce concept en opérant un déplacement de la
détresse psychologique insupportable à limpulsion sexuelle insupportable.
Actuellement, peu de neurologues et même peu de psychiatres qui soccupent de
ces patients nadhèrent à ce concept.
Durant le XXe siècle, lhystérie a fait lobjet dun manque dintérêt certain,
en comparaison avec le développement des autres pathologies neurologiques et
psychiatriques, et ceci à la fois de la part des neurologues et des psychiatres.
Il y a plusieurs raisons possibles:
1) durant la Grande guerre il y a eu une sorte dépidémie de phénomènes
hystériques chez les soldats en rapport avec des situations extrêmes sur le
champ de bataille. Les neurologues ont utilisé des méthodes barbares pour
essayer de traiter ces patients quils avaient du mal à comprendre. Peut-être
ont-ils voulu dune certaine manière oublier cette période difficile (voire dans
le menu déroulant « patients » le texte sur la Grande guerre)
2) les neurologues ont du mal à reconnaître comme patient « neurologique » des
patients qui ont des symptômes fluctuants et incongrus par rapport aux symptômes
rencontrés dans les pathologies neurologiques classiques. Ne pas respecter les
règles des corrélations anatomo-cliniques élaborées sur plusieurs siècles par
les neurologues, pouvait être considéré comme insupportable. Cependant, on verra
ci-dessous, dans les exemples de patients que nous allons donner, que ces
symptômes dit « incongrus » peuvent avoir une cohérence avec certains modèles
physiopathologiques des TNF
3) Le développement considérable de lidentification des pathologies
neurologiques grâce aux techniques dimagerie, dexamens biologiques, génétiques
et danatomopathologie a laissé peu de place pour ses patients hystériques qui
ne se laissent pas appréhender par les examens complémentaires.
THEORIES ACTUELLES
Le début du changement conceptuel actuel date dune dizaine dannées et il a été
initié par nos collègues neurologues britanniques. Ils ont étudié de grandes
séries de patients avec TNF, leurs symptômes, les modes de déclenchement et leur
évolution. Le déclenchement des symptômes par un facteur psychologique nest
plus considéré comme indispensable. Un traumatisme physique peut entraîner ce
type de troubles sans quil ny ait aucune psychopathologie associée. Dans ces
séries de patients, le pronostic global de ces troubles est défavorable même sur
des études menées sur le long terme à 12 ans. Ces neurologues considèrent que
les paralysies ont le même pronostic global que la sclérose en plaques, que les
mouvements anormaux fonctionnels ont le même pronostic que les
maladies dégénératives des noyaux gris, que les crises non-épileptiques ont une
évolution parfois plus grave que lépilepsie elle-même. Ils ont bien montré que
considérer ces malades comme atteint dune pathologie psychiatrique aggrave la
situation. Ils proposent de considérer ces malades comme ayant problème
neurologique avec une perturbation du « software » cérébral, sans négliger pour
autant lapproche psychologique nécessaire chez beaucoup de patients. Le terme
de troubles neurologiques fonctionnels (TNF) a été proposé pour insister sur
limportance de lapproche neurologique chez ses malades.
Les TNF sont maintenant considérés comme la conséquence de modification de la
connectivité cérébrale (lensemble des connections entre les neurones
cérébraux). Mais plusieurs modèles explicatifs existent actuellement pour
expliquer comment un traumatisme physique, une affection médicale ou un
événement psychologique va produire des troubles neurologiques fonctionnels
1) Le modèle Bayésien
Le modèle le plus couramment admis actuellement est celui élaboré par
Mark Edwards. Il se réfère au modèle Bayésien du fonctionnement cérébral. Le
cerveau fonctionne comme un ordinateur dans lequel se construit progressivement
un modèle interne du monde qui va permettre dinteragir par des prédictions à
partir des informations sensorielles que le cerveau va recevoir. Pour chaque
information reçue, il y a une anticipation ou une prédiction par inférences
statistiques, le plus souvent inconsciente, sur la nature de cette information.
Dans ce modèle, le cerveau va générer en permanence de telles anticipations. Ce
système permet de gagner du temps en disposant dinformations à lavance.
Lorsque ces prédictions sont violées par des entrées sensorielles inattendues,
Il va déclencher un signal de surprise ou derreur. Les événements déclenchant
les troubles fonctionnels vont modifier le modèle interne du monde et par voie
de conséquence, modifier les idées et les prédictions sur les informations
reçues, entraînant des troubles de lattention focalisées et des perturbations
des perceptions et des mouvements. Le traitement qui découle de cette théorie,
consistera essentiellement, par thérapie cognitive, à essayer de normaliser les
représentations supposée être à lorigine des troubles. (pour plus
dinformations voir le lien avec la video du Dr M Edwards et sa traduction)
2) Le modèle « dissociatif »
Il existe actuellement une autre théorie, moins couramment adoptée, mais
qui paraît plus cohérente avec le mode daction supposé et les résultats de la
stimulation magnétique. Cette théorie a été introduite par Pierre Janet à la fin
du XIX° siècle. Il fait référence à un processus psychobiologique par lequel,
sous leffet dune émotion ou trauma psychologique intense, le fonctionnement
cérébral va se dissocier, se fragmenter, se compartimentaliser et serait à
lorigine des différents symptômes neurologiques fonctionnels. Il appelle ce
phénomène « dissociatif » Ce processus serait non lésionnel (fonctionnel) et
potentiellement réversible. Il pourrait être la conséquence de troubles de la
connectivité que lon commence à voir en imagerie fonctionnelle dans certains
centres de recherche. Les comportements ou processus, que nous voulons
effectuer, sont coupés de la conscience par un rétrécissement du champ de la
conscience (trouble du monitoring) ou du système exécutif (trouble du contrôle).
Nous verrons ci-dessous quun traumatisme, non pas psychologique, mais physique
focalisé peut très probablement être à lorigine dun phénomène dissociatif au
niveau des réseaux neuronaux correspondants et entraîner en retour un trouble
fonctionnel neurologique.
Pour illustrer ce phénomène dissociatif, une étude de P Vuilleumier à Lausane
montre que dans les déficits sensori-moteurs unilatéraux fonctionnels, il existe
une hypoactivité des boucles cortico-sous-corticales de la région centrale
controlatérale et qui disparait lorsque le patient guéri.
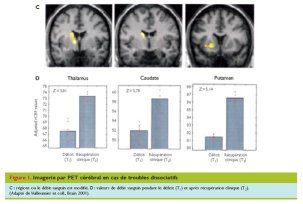
Une autre étude de V. Voon à Londres montre que chez ce type de patients, il existe une déconnexion entre laire motrice supplémentaire qui est très importante dans la programmation des mouvements et les régions préfrontales, entraînant une inhibition de la motricité volontaire. Il existe, cependant une hyperactivité des régions limbiques (cerveau émotionnel), traduisant limportance des phénomènes psychologiques chez nombre de ces patients.

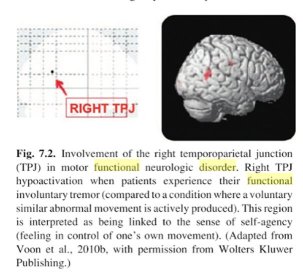
Cette même chercheuse a montré un dysfonctionnement à type dhypoactivation au niveau de la jonction temporo-pariétale droite responsable de lagentivité, processus par lequel on a conscience que lactivité quon réalise a été planifiée par nous et quelle nous appartient.
Les TNF sont souvent appelés «
troubles neurologiques fonctionnels et dissociatifs ». Le sens du mot
dissociatif donné actuellement à ces troubles est différent de celui proposé par
P. Janet. Dans lutilisation actuelle, il fait référence à des états où le sujet
peut se trouver déconnecté par rapport à son corps et éprouver un sentiment de
dépersonnalisation (il se sent bizarre, déconnecté, être à la fois là et pas
la). Il fait également référence à des états où le sujet peut se trouver
déconnecté par rapport à son environnement et éprouver un sentiment de
déréalisation (son entourage lui paraît loin et irréel comme sil planait. Il se
sent distant de son entourage). Pour Pierre Janet, tous les symptômes des TNF
sont liés à des processus dissociatifs.
Dans ce modèle, il est possible que la stimulation magnétique trans-crânienne «
large champ » et périphérique puissent agir sur ces troubles de la connectivité
et rétablir un fonctionnement cérébral normal.
3) Le modèle du trouble proprioceptif
Les recherches sur les facteurs prédisposant aux TNF se sont orientées
uniquement sur les caractéristiques psychopathologiques des patients. Dans ce
modèle, les TNF seraient essentiellement la conséquence dun déficit
dactivation des capteurs proprioceptifs périphériques situés dans le tissu
conjonctif vers le cerveau. Ces capteurs proprioceptifs renseignent en
permanence le cerveau sur létat du corps. Ce déficit serait lié à un
dysfonctionnement de ces capteurs en rapport avec une altération génétique
tissus conjonctif observé chez la grande majorité de ces patients (voir page «
TNF et syndrome dEhlers Danlos »). Le tissu conjonctif assure larmature de
presque tous les organes. Pour cette raison, le cerveau est mal et
insuffisamment renseigné et stimulé. En retour, cela crée des tensions
musculaires, de la douleur et des troubles du contrôle de nombreux organes
(commande motrice, colopathie fonctionnelle, troubles vésicaux, de la
vasomotricité, etc..). Ce manque de stimulation cérébrale est aussi probablement
à lorigine de la fatigue qui est présente chez tous ces patients, des troubles
cognitifs associés (mémoire de travail, attention, difficulté à trouver ses mots
etc.), déventuels malaises, par lintermédiaire dune possible déconnexion
cérébrale secondaire. Ce trouble proprioceptif favoriserait donc des phénomènes
« dissociatifs » tels quils sont décrits dans le modèle précédent. Pour cette
raison, ces patients sont prédisposés à subir des TNF lors dune perturbation
physique ou émotionnelle plus ou moins importante et parfois subtile. En effet,
linterrogatoire et lexamen clinique des patients avec TNF permettent très
souvent (environ 3 patients sur 5 et encore plus fréquemment dans la
fibromyalgie) de mettre en évidence des éléments en faveur une de
cette fragilité constitutionnelle du tissu conjonctif qui caractérisent le
syndrome dEhlers Danlos « hypermobile » ou, selon la classification
internationale de New York (2017), les troubles du spectre de lhypermobilité (HSD
pour Hypermobile Spectrum Disorders). Les capteurs proprioceptifs
périphériques par stimulation magnétique périphérique et dagir sur la
connectivité cérébrale par stimulation magnétique centrale cérébrale transcranienne large champ. Les facteurs prédisposant des TNF seraient donc
essentiellement dorigine somatique, même si des perturbations
psychopathologiques peuvent aggraver cette prédisposition ou être lélément
déclencheur.